




Please click the frequently asked questions below for further information and IPC precautions required:
-
What is TB?
It is caused by organisms of the Mycobacterium tuberculosis complex, including M. tuberculosis, M. bovis and M. africanum. All three of these organisms are capable of causing TB in humans.
The risk of infection depends upon duration of exposure, the intensity of the exposure, and the immune status of the person exposed. The immune system clears the bacteria immediately in more than 80% of people exposed.

TB can present in a number of different ways. The most common are listed below:
Latent TB
In a small proportion of people who have been infected, the bacteria are walled off and remain dormant but viable. This is called latent TB. It is estimated that 5-10% of those with latent TB will develop active TB during their lifetime. Patients with latent TB are not considered infectious.
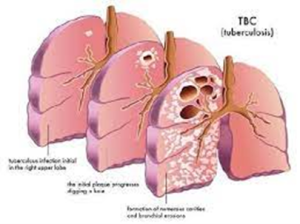
Active Pulmonary TB
The most infectious form of TB is pulmonary TB, particularly smear positive cases where TB bacilli can be seen on direct microscopic examination of the sputum. Left untreated, it is estimated that each person with active TB will infect on average between 10 and 15 people each year.
Closed TB
Non-pulmonary TB is less common than the pulmonary form and can involve any organ or tissue, most commonly bone, lymph nodes, central nervous system, skin and the genito-urinary tract. Patients with closed TB are not deemed to be infectious unless the infected area is disturbed, usually through an invasive procedure including surgery or open wound.
Multi Drug resistant TB (MDR-TB)
Sometimes drug-resistant TB occurs when bacteria become resistant to the drugs used to treat TB. This means that the drug can no longer kill the TB bacteria.
Drug-resistant TB is spread the same way that drug-susceptible TB is spread.
Extensively drug resistant tuberculosis (XDR-TB)
XDR-TB is a rare type of MDR-TB that is resistant to the most potent TB drugs. Patients are left with treatment options that are much less effective. XDR-TB is of particular concern for persons with HIV infection or other conditions that can weaken the immune system.
-
Why is this information important?
If NIAS staff are aware that the patient has a suspected or confirmed case this should be communicated to the Control Room (Emergency or Non-emergency as appropriate) and the staff in the receiving unit when transferring the patient to ensure effective patient care and management.
Early risk assessment for TB and the presentation of the TB ensures staff can use appropriate PPE is worn to prevent staff exposure.
The IPC Team should be contacted if there is concern regarding a confirmed or suspected case of TB.
-
How is it spread?
Pulmonary TB is considered the most infectious as it is spread through the air from one person to another called an Airborne Route. When a person with TB disease of the lungs or throat coughs, speaks, or sings, TB bacteria can get into the air. People nearby may breathe in these bacteria and become infected.
When a person breathes in TB bacteria, the bacteria can settle in the lungs and begin to grow. From there, they can move through the blood to other parts of the body, such as the kidney, spine, and brain.
People with TB disease are most likely to spread it to people they spend time with every day. This includes family members, friends, and coworkers or schoolmates.
Closed TB: The TB becomes infectious if the affected area is disturbed and aerosolised during invasive procedures. Eg: spinal surgery if the TB is located in the spine.
-
What are the symptoms of TB?
Symptoms of TB disease depend on where in the body the TB bacteria are growing.
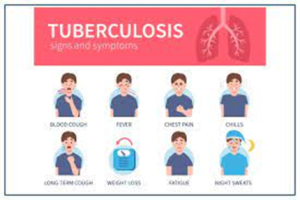
TB disease in the lungs may cause symptoms such as:
- a bad cough that lasts 3 weeks or longer
- pain in the chest
- coughing up blood or sputum (phlegm from deep inside the lungs)
Other symptoms of TB disease are:
- weakness or fatigue
- weight loss
- no appetite
- chills
- fever
- sweating at night
Symptoms of TB disease in other parts of the body (Closed TB) depend on the area affected.
People who have latent TB infection:
- do not feel sick,
- do not have any symptoms, and
- cannot spread TB to others.
-
IPC Precautions
- Airborne Precautions should be used for Pulmonary TB and Closed TB if the affected area is disturbed/open.
- Hand Hygiene should be completed as per the 5 moments in line with usual practice.
- Eye protection should be worn
- FFP3 Mask should be worn
- Gloves and Aprons should be worn.
- The patient should be transported via ambulance with no other patients present.
- The patient should be asked to wear a Fluid Resistant Surgical Mask unless there is concern about MDR-TB which should be discussed with the IPC team. (If tolerated and does not interfere with their treatment needs)
- Laundry should be treated as contaminated, placed into an alginate bag and placed into a red laundry bag.
-
Do staff need any prophylaxis or follow up?
You may have been exposed to TB bacteria if you spent time near a patient with active pulmonary TB disease or closed TB if the area is exposed such as an open wound / surgical site. Follow-up of contacts is determined by whether appropriate PPE was used and what type of TB you have been exposed to.
If you believe you have been in contact with a known case of TB contact your line manager immediately and the IPCT at the earliest convenience who will complete a risk assessment and if required a referral to Occupational Health will be made. They will then complete a risk assessment.
No Follow-up is required of contacts where appropriate PPE was used.
Follow-up of contacts where appropriate PPE was not used:
If you were exposed to a patient with a confirmed Pulmonary TB or to closed TB where the site is open such as a surgical site then you should contact your line manager and the IPC team during working hours.
It is important to note that there is no immediate risk to staff and no action immediate staff follow up is required out of hours.
It is important to know that a person who is exposed to TB bacteria is not able to spread the bacteria to other people right away. Only persons with active TB disease can spread TB bacteria to others.
Following a risk assessment you may be asked to contact Occupational Health for follow up which may include a blood test, chest x-ray and BCG check.
-
What cleaning is required?
All equipment and the ambulance should have a between patient clean paying particular attention to touch points.
Where possible leave the doors of the ambulance open while patient is being transferred to the receiving unit.
- Links to Guidance